
Knee Bursitis Treatment for Pickleball and Tennis Players in Sarasota

Knee Bursitis in Pickleball and Tennis Players: Why the Knee Is Usually Not the Whole Problem
If you play pickleball or tennis regularly and you're dealing with knee swelling, tenderness at the front of the kneecap, or pain that flares after matches and stiffens overnight, you're likely dealing with prepatellar bursitis. It's one of the more common presentations we see in court sport athletes, and it tends to be stubborn when it's treated as an isolated knee problem, because it usually isn't one.
What's Actually Happening in the Knee
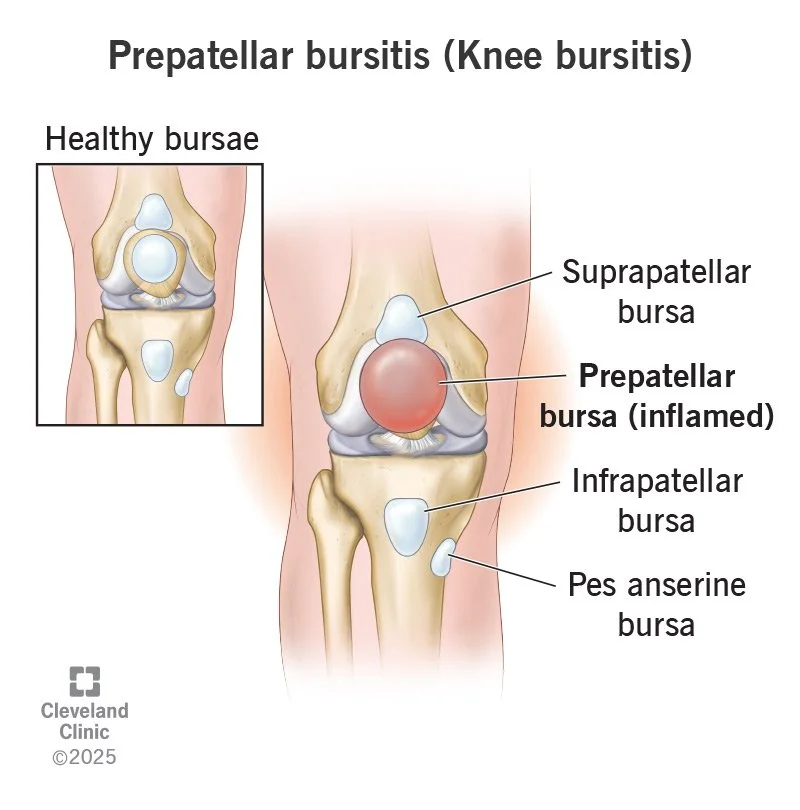
The prepatellar bursa is a small fluid-filled sac that sits in front of the kneecap. Its job is to reduce friction between the patella and the surrounding tissue. When it becomes inflamed, it fills with fluid, causing the characteristic swelling, warmth, and localized pain just above or over the kneecap.
In court sport athletes, this typically develops through repetitive microtrauma. The lateral cuts, split steps, quick direction changes, and repeated knee flexion that pickleball and tennis demand place sustained mechanical stress on the bursa over time. Left unaddressed, the inflammation becomes chronic. Fibroblast proliferation and fibrin deposition can lead to thickening and fibrotic adhesions within the bursa, which makes it harder to resolve and more likely to recur.
The pain itself has a biochemical component too. Persistent inflammation triggers nociceptor sensitization, which is why the knee can feel tender and reactive even with relatively low levels of activity. The tissue becomes progressively more sensitized, and the pain starts to feel disproportionate to what you're actually doing.
Why Treatment Focused Only on the Knee Often Stalls
The bursa is irritated, but the reason it's being overloaded usually comes from somewhere else in the kinetic chain.
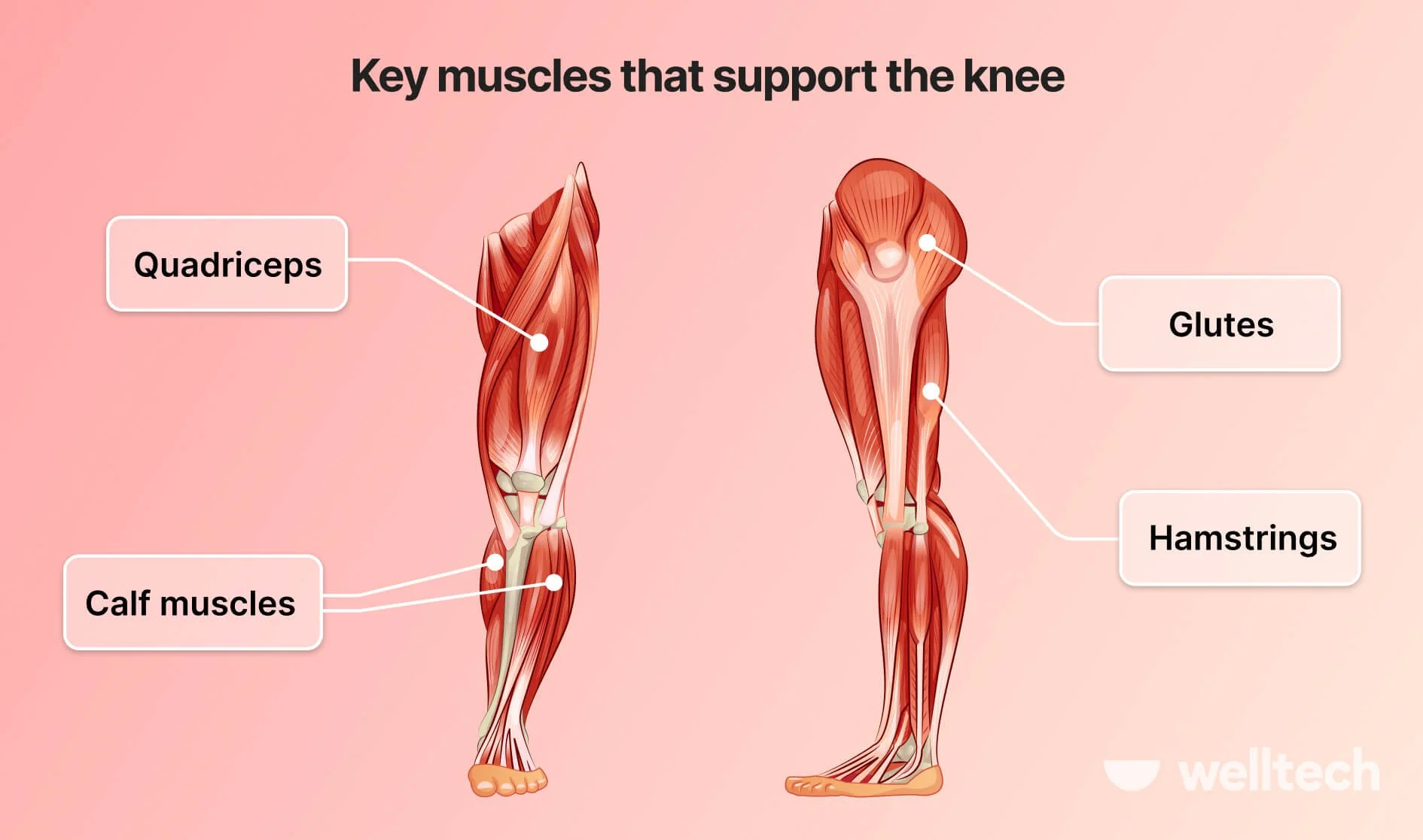
In court sport athletes specifically, we consistently find contributing factors in the hip, quad, and foot that are driving excess load into the knee. Tight hip flexors and restricted hip internal rotation alter how force transfers through the lower limb during lateral movement. When the hip can't absorb and distribute load properly, the knee takes more than its share. Quadriceps tightness and adhesions in the vastus lateralis change how the patella tracks and how the knee loads through flexion. Foot mechanics matter too. A collapsed arch, restricted ankle dorsiflexion, or poor contact pattern during the push-off phase of a split step can shift ground reaction forces up the chain directly into the knee.
On top of that, gait and movement patterns that develop around pain tend to become habitual. Players start loading one leg differently, favoring one side of the court, or modifying their footwork without realizing it. These compensations reduce pain in the short term but increase load asymmetry and make the underlying problem harder to resolve.
How We Treat It at Well Co
Our approach covers the bursa itself and everything feeding into it.
For the bursa, StemWave focused shockwave therapy is the primary treatment tool. It delivers high-energy acoustic pulses into the inflamed tissue:
→ downregulating the pro-inflammatory cytokines driving the chronic irritation
→ stimulating new blood vessel formation for improved circulation
→ activating the repair mechanisms that allow the tissue to remodel.
Most patients notice a reduction in swelling and tenderness within two to three sessions. Range of motion and functional movement follow as the inflammation clears and the tissue starts to recover its normal properties.
In conjunction with StemWave, we use Active Release Technique to address the soft tissue restrictions contributing to the problem. In knee bursitis presentations in court athletes, that typically means working through the quadriceps, with particular attention to the rectus femoris and vastus lateralis, the hip flexors, the glutes and external rotators, and the plantar fascia and calf complex. These aren't just tight muscles sitting adjacent to the problem. They're structures whose restrictions are actively changing how load moves through the knee on every step, every lunge, and every split step you take on the court.
We also look at gait and movement patterns. For pickleball and tennis players, that means assessing how you're loading through stance and push-off, how your lateral movement is distributing force, and whether any compensatory patterns have developed around the knee pain. Where we find them, we address them directly, both in the treatment and in the home program we build for you.

Your Home Program
What you do between sessions determines how quickly the tissue recovers. We put together a home program specific to your presentation, typically including hip mobility work, quad and posterior chain loading progressions, and movement drills that reinforce better mechanics during court-specific patterns. The goal is to support what we're doing in the clinic and reduce the cumulative load the knee is absorbing during your regular activity.
We don't ask patients to stop playing entirely unless the presentation requires it. For most court athletes, modifying volume and intensity temporarily while the tissue responds to treatment is enough. Getting you back on the court at full capacity, without the knee flaring after every match, is the point.
What to Expect
Most patients see meaningful improvement within two to three weeks of starting care, typically one to two sessions per week. Cases with significant chronic changes or long-standing compensatory patterns take longer, but a clear trajectory of improvement should be visible early. We give you an honest picture of your timeline at the first visit based on what the assessment shows.
If you're a pickleball or tennis player in Sarasota dealing with knee bursitis that hasn't resolved with rest or anti-inflammatories, we're at 3982 Bee Ridge Rd, Sarasota, FL 34233. Book online at wellcochiropractic.com or call to schedule.